 |
Considering a patient’s contact lens options based solely on their diagnosis is easy. While this may result in acceptable fits for a reasonable percentage of patients, each patient deserves individualized care despite what might be a common condition. This is especially evident with irregular cornea patients, where one size does not fit all. This case looks at a rarely used lens option in keratoconus fitting, a bitoric corneal gas permeable, and illustrates why this specific design presented the best contact lens option for this particular patient.
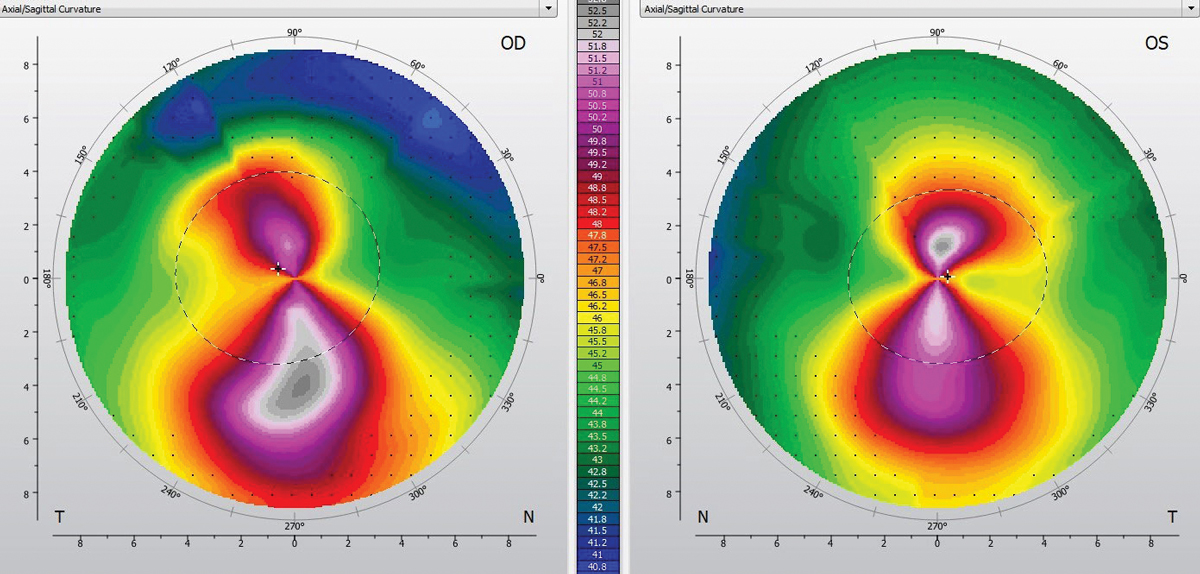 |
Fig. 1. Note the relatively symmetrical, with-the-rule astigmatic pattern in the left eye. Click image to enlarge. |
The Case
A 54-year-old Hispanic male was referred for a contact lens evaluation by his corneal specialist. The patient was diagnosed with keratoconus in his mid-teens and was first prescribed polymethyl methacrylate contact lenses and, later, gas permeable contact lenses. He struggled with decreased wear time and discomfort in the left eye while wearing his gas permeable contact lenses, which had worsened over the past several years to the point where he discontinued lens wear about two months prior to the appointment.
A manifest refraction of -6.50-3.75x015D OD and -6.50-4.25x170D OS yielded distance visual acuities of 20/30-2 OD and 20/20-2 OS. Corneal findings consistent with mild keratoconus demonstrated a Fleischer ring, apical thinning and Vogt’s striae in both eyes. Fortunately, no corneal scarring was present in either eye. Topography displayed an asymmetric with-the-rule appearance with more asymmetry and axis variance in the right eye than the left. Centrally, the left eye was fairly regular (Figure 1). Elevation maps displayed a fairly common inferior depression below the cone of the right eye. The left eye, however, displayed a relatively symmetrical elevation map with comparable superior and inferior depression (Figure 2).
I discussed contact lens options with the patient with a particular emphasis on corneal gas permeable, hybrid, scleral and custom soft lenses. The patient was reluctant to consider options beside corneal gas permeable lenses, as he felt he would have difficulty adjusting to the change.
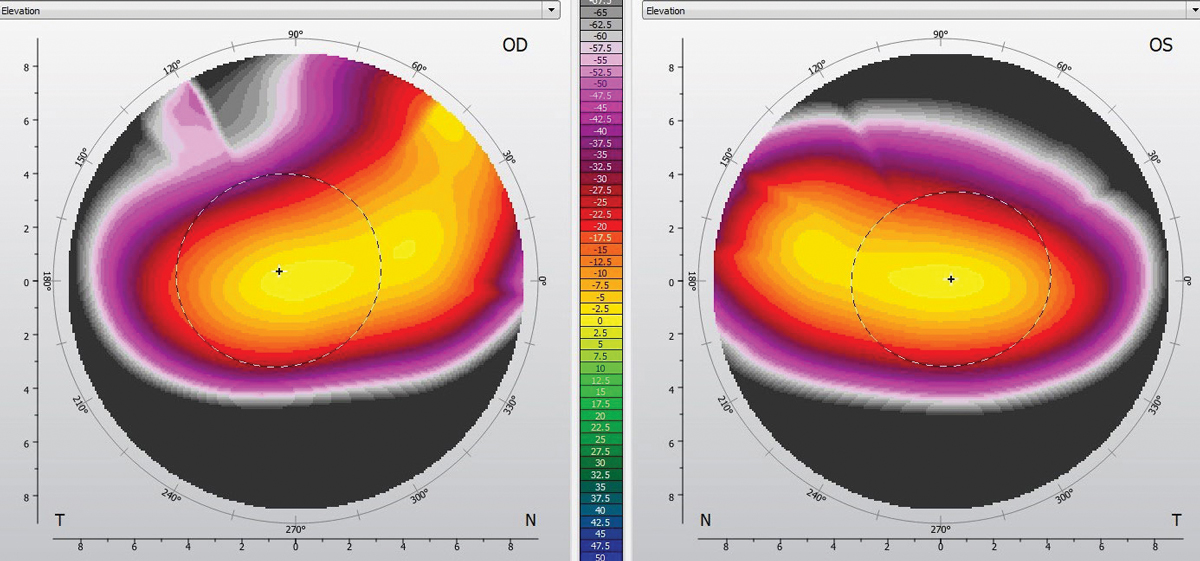 |
Fig. 2. Symmetrically superior and inferior depression is evident in the left eye. Click image to enlarge. |
Diagnostic Fitting
I trialed a gas permeable keratoconus design with a moderate-sized diameter on each eye. In the right eye, a diagnostic lens of -3.00D, base curve radius of 6.96mm and overall diameter of 9.50mm helped achieve a central three-point-touch pattern. I observed excess inferior edge lift and ordered a lens with inferior tuck, or quadrant-specific inferior steepening, to lessen inferior edge lift and aid centration. An over-refraction of -4.50D provided 20/20 vision in the right eye.
In the left eye, I had difficulty identifying a lens with an acceptable fluorescein pattern and centration. I observed an evident with-the-rule fluorescein pattern (i.e., bearing along the horizontal meridian, clearance along the vertical meridian), as well as excess movement with blink and inferior decentration. While steepening the base curve improved alignment in the horizontal meridian, it created excess clearance along the vertical meridian. Based on the fluorescein pattern observed with the spherical lens and the relative symmetry observed in both the topography and elevation maps, a toric back-surface lens was preferable.
I used diagnostic fitting information to determine the right lens parameters and ordered the left lens empirically. The right lens had a power of -7.25D, base curve radius of 6.96mm, overall diameter of 9.50mm, standard edge lift and two steps of inferior edge tuck. The left lens had a power of -5.75/-8.50D, base curve radius of 44.25/47.75mm, overall diameter of 9.50mm and axial edge lift of 0.12mm.
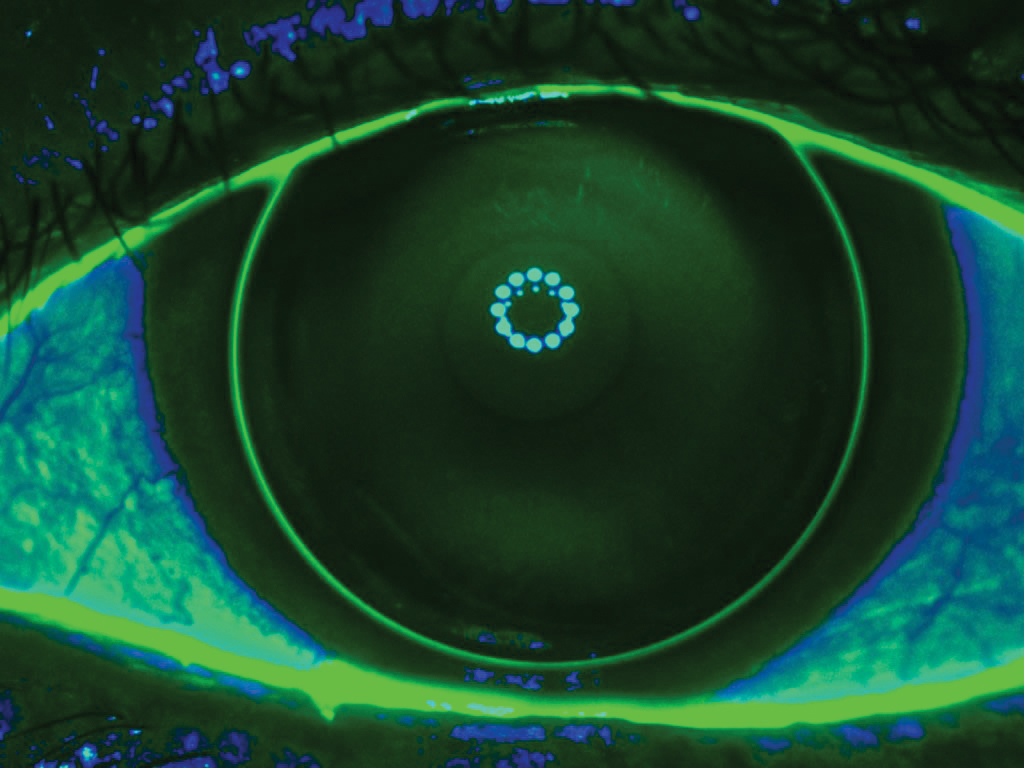 |
| Fig. 3. This bitoric lens has a central three-point-touch fluorescein pattern. Click image to enlarge. |
Lens Dispensing
With the ordered lenses, distance visual acuities were 20/20 OD, OS and OU. Slit-lamp evaluation of the right lens displayed a central three-point-touch pattern and average/uniform edge lift. The inferior edge lift had improved as a result of the inferior tuck. The left eye’s lens was centered and displayed a three-point-touch pattern with a feathered touch centrally that increased to paracentral clearance and returned to a mid-peripheral touch pattern (Figure 3). I deemed the edge lift inadequate, so I reordered it with an increase in axial edge lift from 0.12mm to 0.16mm. The new fit was satisfactory, and both lenses were dispensed.
Follow-up
The patient returned one week later wearing his contact lenses. He reported improving comfort with a gradual return to lens wear. He also noted excellent vision and equal comfort between the right and left eyes. Distance visual acuities were 20/20 OD, OS and OU. The corneal surface was intact and tolerating lens wear adequately.
At the six-month follow-up, the patient had increased lens wear from 12 to 16 hours each day with excellent vision and equal comfort in both eyes. The corneal surface remained intact, and topography showed stable results in each eye.
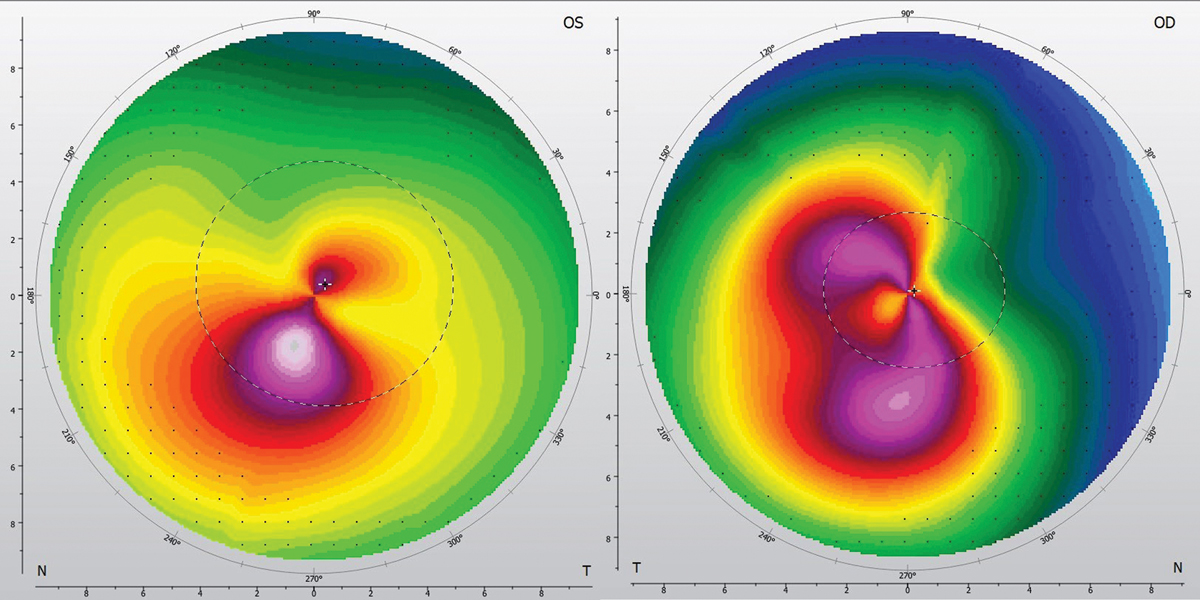 |
Fig. 4. Superior-inferior asymmetry (left) and principal meridian variance. Click image to enlarge. |
Discussion
Several options exist when fitting patients with keratoconus, including corneal gas permeable, hybrid, scleral and custom soft lenses. Within the family of corneal gas permeable lenses, clinicians can achieve successful fitting relationships in a wide range of diameters, depending on the size and location of the cone. Smaller and more central cones may benefit from smaller-diameter lenses, while lower or larger cones may see improved fits with larger-diameter or intralimbal designs.1
Due to the anterior surface irregularity typically present in keratoconus, bitoric lenses are rarely applicable. For a bitoric to be considered, a high degree of inferior/superior symmetry must be present. In addition, a bitoric lens performs best when the principal meridians of the eye are located 90° apart.
To help you visualize these two criteria, imagine a figure eight. Comparing the size and shape of the top and bottom of the pattern helps to reveal its symmetry. If the principal meridians are not 90° apart, the pattern will be skewed so the top and bottom of the figure eight don’t stack directly on top of each other (Figure 4).
For the patient in this case, each eye dictated its own lens design. The more asymmetric right eye was able to achieve a fit in a moderate-diameter, keratoconus-specific corneal lens. Due to the toric yet symmetrical nature of the left cornea, a back-surface toric lens was necessary to improve centration and the central fitting relationship. By considering the individual characteristics of each eye, clinicians can create clear and comfortable contact lenses.

