 |
A 53-year-old female with a history of bilateral myopic LASIK, performed in 1992, was referred with epithelial ingrowth OU. She previously underwent enhancement procedures in each eye (radial keratotomy OS, astigmatic keratotomy OU) and had a flap lift for epi ingrowth OD 10 years prior. She complained of decreased vision (OD>OS) but denied pain, discomfort or irritation.
Post-LASIK epithelial ingrowth is a rare complication characterized by the ingrowth of corneal epithelium at the interface between the flap and stromal bed. It has been reported in up to 3.9% of patients after initial surgery but up to 20% if the flap is lifted for retreatment.1 While most cases are self-limited, surgical treatment is required in 0.92% to 3.2% of patients when cells extend into the visual axis and reduce vision, induce astigmatism and/or cause keratolysis or foreign-body sensation.1
Risk factors include type of refractive correction (hyperopic>myopic), surgical instrumentation (microkeratome>femtosecond), retreatment, location of flap hinge, corneal epithelial injury, flap dislocation, type 1 diabetes, epithelial basement membrane dystrophy and possibly increasing age.1
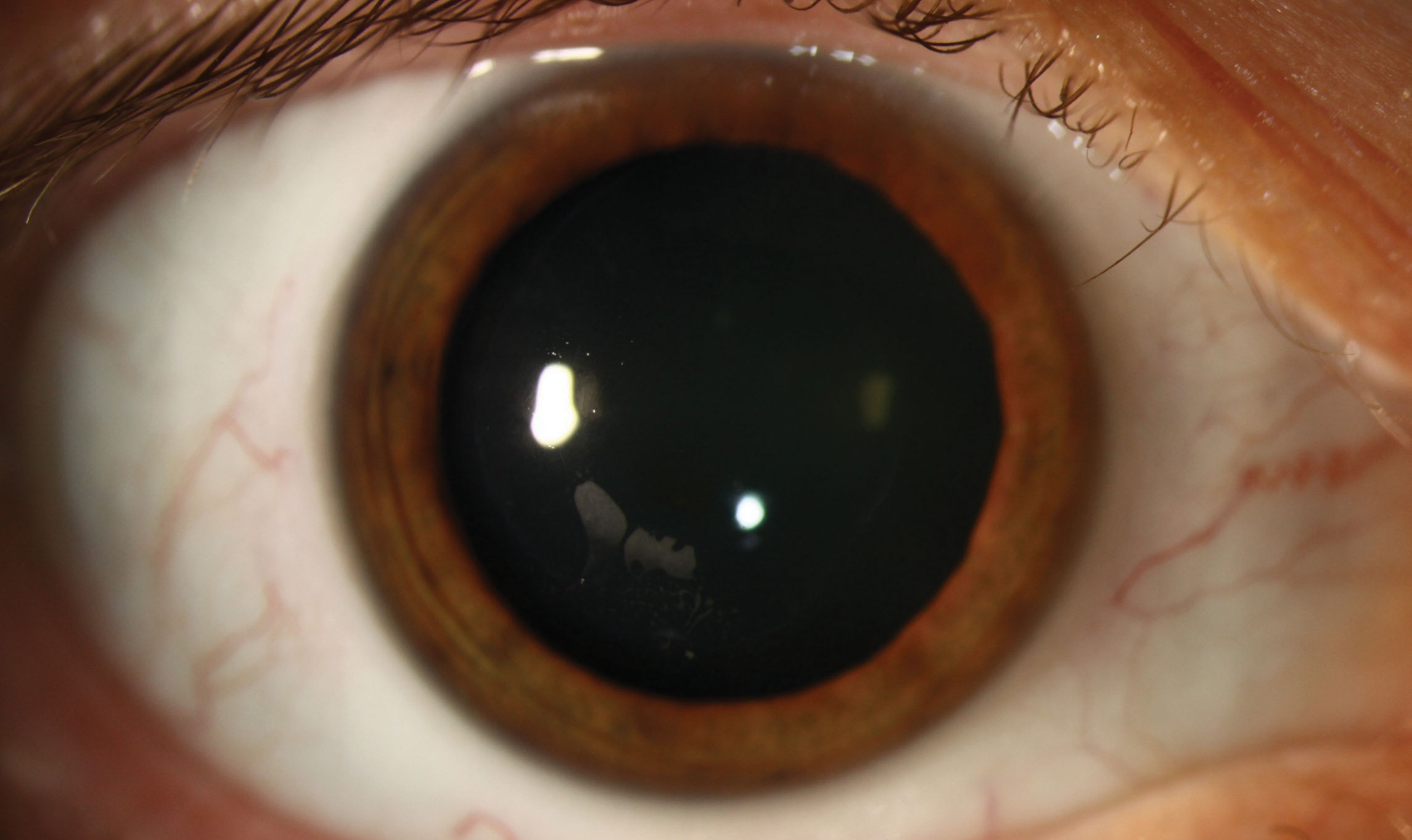 |
| This patient has post-LASIK epithelial ingrowth, a rare complication characterized by the ingrowth of corneal epithelium at the interface between the flap and stromal bed. Click image to enlarge. |
Ingrowth is staged into four categories. Stage 1 is non-progressive; one to two cells within 2mm of the flap edge with a well-delineated white line on the advancing edge. Stage 2 has thicker cell growth with no demarcation line; the leading edge of the flap is rolled or grey with no melt. Stage 3 has thick ingrowth with geographic areas of necrotic cells more than 2mm from the flap edge, with no demarcation line; the flap is rolled with a thickened, whitish-grey appearance. Stage 4 shows aggressive growth and strands of epithelial cells near the visual axis. As there is concern for flap melt, it requires urgent treatment.2
The most common intervention is mechanical debridement of the flap-stromal interface. Amniotic membrane graft may be used in cases associated with flap injury or melting.
Our patient was diagnosed with Stage 1 epithelial ingrowth and surgical treatment was deferred. She was referred for contact lens fitting to help with her blurred vision.
1. Ting DSJ, Srinivasan S, Danjoux JP. Epithelial ingrowth following LASIK: prevalence, risk factors, maangement and visual outcomes. BMJ Ophthalm. 2018 Mar 29;3(1). 2. Yesilirmak N, Chhadva P, Cabot F, et al. Post-LASIK epithelial ingrowth: treatment, recurrence and long-term results. Cornea. 2018;37(12)`51`7-21. |

