There’s been an increased focus on myopia management in recent years and, as primary eye care providers, optometrists are positioned at the forefront of this effort. The shift is largely due to the growing prevalence of myopia as well as new research breakthroughs. In North America alone, cases grew by 6.2% between 2000 (28.3%) and 2010 (34.5%) and are expected to reach 58.4% by 2050. Worldwide, it’s projected that the prevalence will be 49.8% by 2050, meaning five billion people will be myopic and nearly one billion of those individuals will develop high myopia.1
“In the past three decades, we have witnessed an increasing global prevalence of myopia that trends suggest will continue,” notes Kevin Chan, OD, senior clinical director at Treehouse Eyes of Vienna, VA. “We are also expecting to see a surge of myopia in children, which is why it is so important to engage in myopia management when patients are still young, and we actually have the best chance to slow progression.”
Current myopia control options include atropine drops, soft multifocal contact lenses and orthokeratology lenses. Multifocals for myopia management, a relatively new area of care, is seeing increased interest, but has not yet been widely adopted. This article will explore this service and not only how ODs can integrate it into their practice, but how to do so successfully.
 |
|
Pervasive digital device use among kids—and their consequent reduction in time outdoors—is accelerating myopia onset in younger populations. Photo: Getty Images. Click image to enlarge. |
Multifocals for Myopia
A number of studies have explored multifocal contact lens and their role in myopia management. One of the most recent, the Bifocal Lenses in Nearsighted Kids (BLINK) randomized clinical trial, sought to determine if center-distance soft multifocal contact lenses slow myopia progression in children when compared to single-vision lenses. It also examined whether high add power (+2.50D) slows myopia progression more than medium add power (+1.50D).2 The Biofinity lens from CooperVision was used in the study.
The BLINK study, a three-year clinical trial, recruited 294 school-aged myopes without any signs of pathological myopia.3 Throughout the course of the study, the children wore contact lenses daily and had yearly exams. Findings showed that high add power multifocal contact lenses significantly reduced the rate of myopia progression when compared to single vision contact lenses of the same power and medium add power multifocal lenses. The BLINK study is now in second phase and participants will wear the +2.50D add for the next two years followed by single vision lenses for the final year of the study.3
Given the evidence supporting this approach as well as a growing need among patients, optometrists must be prepared to navigate myopia management. “As the primary eye care provider, optometrists must take the lead when managing these patients,” notes Maria Walker, OD. PhD, an instructor at the University of Houston College of Optometry. “It is well within our scope of practice and something that we as a profession should take ownership of.
“Using multifocal contact lenses in this way is becoming more mainstream but, like anything new, it takes time to integrate,” she continues. “However, given the overwhelming data and an increasing number of optometrists tackling this aspect of patient care, this is something that everyone can learn to do with confidence.”
 |
| Image: Coopervision. Click image to enlarge. |
Successful Integration
Incorporating this service into your practice begins with the basics: learning more about the various products currently on the market. This starts with education and familiarizing yourself with your options as well as reaching out to representatives of different contact lens manufacturers.
“Doctors need to be more proactive when it comes to doing research, connecting with brands and learning about different products,” says Dr. Chan. “Because just like in other areas of care, there are a variety of new lenses that can be used for myopia control that could offer better vision quality for young patients.”
A thorough understanding of different lens properties and designs is crucial, notes Chris Browning, OD, of Indianapolis, who suggests making a list of the pros and cons of different lenses as well as which children might benefit from which type of design. “ODs should also become familiar with the consulting services of different manufacturers,” he adds. “It is really beneficial to take advantage of consults, especially when integrating this service into your practice.”
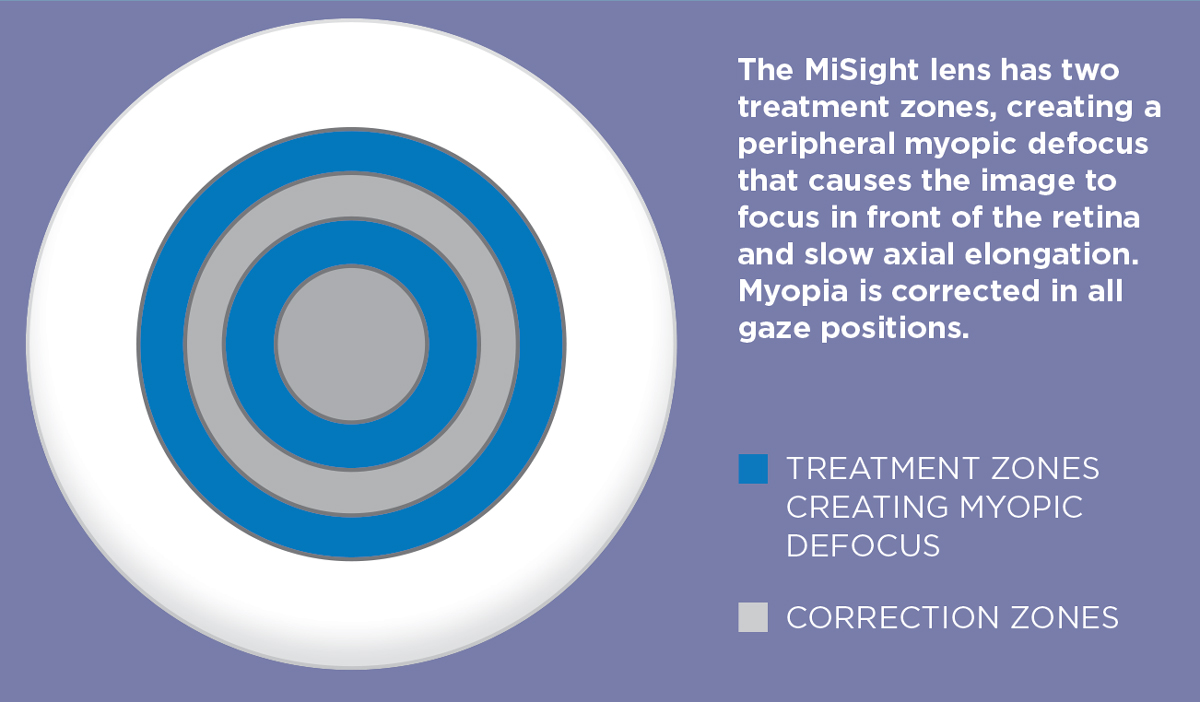
Research suggests the most effective lens design for myopia control is a center-distance multifocal. To date, the only FDA-approved lens for myopia control is MiSight from CooperVision, a single-use, disposable lens is indicated to slow the progression of myopia.4 To get certified to prescribe this lens, ODs must participate in CooperVision’s Brilliant Futures Myopia Management Program, which offers training for physicians as well as tools to support children and their parents.
There are also a variety of lenses that can be used off-label for myopia management, including the Biofinity lens (CooperVision), a one-month replacement daily wear silicone hydrogel lens. It is typically prescribed in both eyes with a +2.50D dominant (center-distance design) add power, according to Andrew Pucker, OD, an assistant professor at the University of Alabama at Birmingham.5 If the patient finds it difficult to adjust to the higher add, a +2.00D dominant add power is sometimes used. “This power seems warranted since the MiSight has been shown to have a meaningful reduction in growth with a +2.00D add,” he notes. Another available option is the NaturalVue multifocal (Visioneering Technologies)—a daily disposable hydrogel contact lens.
There are a number of reasons to select an off-label option, says Dr. Walker, which is why ODs must stay current on the available products. “Cost is often a factor,” she explains. “Also, one lens may fit a patient’s eye better than another. Material, water content, diameter and base curve can all play a role in choosing the right lens.”
The lens modality is also an important consideration, according to Dr. Walker. “Some parents may be more comfortable with a monthly lens rather than a daily lens,” she says. “Certain lenses may match a patient’s lifestyle more than others.”
Once you have determined which option best meets the needs of your patient, ensuring you have the training and tools to properly fit these lenses is paramount to your success. When it comes to selecting power, Dr. Walker suggests that ODs shouldn’t be afraid to put more minus power in the lens than may be predicted based on spherical lens fitting. “Remember, it’s complex optics,” she notes. “Optometrists should feel comfortable using a different power than you would use spherically, as this has been done in clinical trials and the efficacy of the modality is still evident.”
Since MiSight is approved for myopia management, the fitting guide will be an important part of your toolbox. However, off-label lenses will not provide a fitting guide specific to myopia management, notes Dr. Walker. “In those cases, I would encourage you to fit until you are happy with the results. Don’t be afraid, within reason, to go outside the expected parameters. Fit the parameters that allow a patient to see comfortably.” However, Dr. Walker did present a caveat to this—when patients have visually significant residual astigmatism—and discussed consideration of multifocal toric lenses for these patients. When needed, ODs shouldn’t hesitate to prescribe this type of lens, she notes. “There are currently two available options for commercially available soft toric multifocals (CooperVision’s Biofinity toric multifocal and the Ultra Multifocal for Astigmatism from Bausch + Lomb), and of course custom soft lenses are available at most specialty lens manufacturers.”
Practitioners should be mindful that the goal of prescribing multifocal lenses for children “is more than vision correction only; it is largely for managing their myopia progression,” adds Dr. Chan. “At times, some patients may be symptomatic with residual astigmatism at night. Practitioners may need to provide a pair of glasses at a lower prescription as a ‘booster.’”
After an OD has laid the foundation for this new service, the next step is marketing. How are you going to make patients as well as colleagues aware that you now offer multifocal contact lenses for myopia management? Educating current patients is a crucial step. Other marketing tools include social media as well as displaying your services prominently on your website.
“Initially, I think one of the most powerful tools at your disposal is word of mouth,” suggests Dr. Walker. “You don’t have to market loudly. Just start talking about it with your patients. They, in turn, will start discussing it with their friends and family. And as the service grows within your practice, so will your confidence.”
It is never too soon to start the conversation about this service and why it is beneficial to initiate myopia management at an early age, emphasizes Dr. Browning, who makes a point to review the schedule a week in advance and identify patients who have family members who might benefit from this service. “Talk about it with every patient that comes into your practice,” he says. “That includes parents and grandparents. I’ll bring it up with myopic patients who have babies or very young children and even expecting parents, if their child is at an increased risk of developing myopia.”
Making this service standout is another way to highlight its value. “I think that it is important to treat multifocal lenses for myopia management like a referral service,” suggests Dr. Pucker. “You are providing care that goes beyond a standard visit. I would avoid just adding it on to a primary care day; that’s not a good message. Scheduling a standalone visit is important from both a patient perception and billing standpoint.”
Success also depends on a strong support staff, notes Dr. Browning. They are integral to not only building this new service and managing logistics, but also marketing and patient education. “Your staff is key,” he says. “You have to have a team that understands what you’re trying to do and why it is important so they can help execute it effectively.”
Staff buy-in must be a top priority, emphasizes Dr. Walker. “You have to take the time to make sure everyone is on board and is ready to invest their time and energy into this new service. And don’t rush,” she urges. “Take your time to learn what’s working and what’s not working for your practice, then grow from there.”
Clinical Pearls for Myopia Management
|
Patient Buy-In
Another key component of offering any new service is strong patient communication and education, especially in regards to a long-term intervention that comes with a higher price tag.
However, before an OD can effectively communicate the importance of this service to patients and parents, they have to feel comfortable with their own knowledge of myopia management. “We have to step out of our comfort zone and tackle this new area of care,” says Dr. Chan, while suggesting ODs engage in peer-to-peer education and CE opportunities to deepen their understanding of myopia management. “We have to increase awareness and common grounds of knowledge within the eye care community first, before we even have a chance to successfully educate parents.”
When talking to parents, ODs must take the time to thoroughly explain the service and its value. “Patients often think that all soft contact lenses are the same,” explains Dr. Pucker. “You have to help them understand that multifocal contact lenses aim to slow eye growth in addition to correcting distance vision. Fully informing the patient, of what you’re doing and why, is incredibly important.”
Help them understand why this approach is so valuable for their child’s vision and overall well-being. This can be especially useful for the parent who is nervous about a new approach or hesitant due to the cost. Dr. Pucker suggests showing pictures and emphasizing potential outcomes. “The long-term benefit is more than just having less glasses prescriptions in the future,” he says. “It’s also decreasing the risk for vision-threatening conditions, such as retinal detachment, glaucoma and cataracts, in the future.”
Focusing on the long-term benefit also helps parents understand the cost behind this service. “When I talk to parents, I emphasize that this is an investment in their child’s future,” Dr. Browning explains, while noting that his practice works with vendors who allow him to bill patients monthly, which can help ease the financial burden. “We found that patients were much more willing to listen to us when we’re able to break payment down on a monthly basis.”
Taking the time to connect with the child on a personal level can build trust with the patient as well as their patients. It also ensures the child is prescribed the right approach for their personality and lifestyle. “Being able to read the parents as well as the child is very important,” says Dr. Browning. “This requires taking the time to talk to the child. Ask them about their day, their favorite classes and hobbies. Not only does this help you get to know your patient better, it also goes a long way with the parents. They want to feel reassured that you understand their child and their individual needs.”
This can be an intimidating process for the child as well as their parents. By not just jumping into clinical discussions and price points, you are putting them at ease, and they will be more likely to listen to your recommendations with an open mind.
Take-Home Message
Integrating multifocal contact lenses for myopia management into the services you provide is an opportunity to grow your skills and practice exponentially. It is a way to attract new patients while also building a deeper connection with the ones you currently have.
However, to find true success, you have to be prepared to make the commitment, says Dr. Chan. “Invest in education and practice management. Prepare not only yourself as a doctor, but also your staff and practice as a whole,” he notes. “Fully embrace this new specialty if you want to be able to succeed.”
With the growing prevalence of myopia and a greater emphasis on its management, optometrists must take the lead not only for their patients, but also their profession. “The myopia epidemic isn’t going anywhere, so we can either pick up the mantle or wait until ophthalmology takes on the burden,” notes Dr. Walker. “If you want to practice to your full scope as an optometrist, you need to be providing this service. And, if you don’t, you could potentially lose a patient (or family) to another provider.”
As primary eye care providers, optometrists are in the perfect position to offer this important service, which can provide lifelong benefits to patients. And so, the profession as a whole must change their mentality when it comes to myopia management, notes Dr. Browning.
“There is no primary care OD in this country who doesn’t see a myopic child in their practice every day,” says Dr. Browning. “And it’s just too easy to do what we’ve always done—give them a pair of glasses and send them out the door.
“If you aren’t treating the myopia then you need to send them to somebody that is because we now have the knowledge and tools to help these children,” he concludes. “They’re in your chair on a daily basis and we have the chance to change these children’s lives forever. We just have to take it.”
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–42. 2. Cheung N. Myopia: Translating science into practice. Review of Optometry. 2021. www.reviewofoptometry.com/article/myopia-translating-science-into-practice. 3. Walker M. Unpacking the BLINK study. Review of Cornea and Contact Lenses. 2021. www.reviewofcontactlenses.com/article/unpacking-the-blink-study. 4. US Food and Drug Administration. FDA approves first contact lens indicated to slow the progression of nearsightedness in children. 2019. www.fda.gov/news-events/press-announcements/fda-approves-first-contact-lens-indicated-slow-progression-nearsightedness-children. 5. Pucker A. Soft Contact Lens-Based Myopia Management. Review of Myopia Management. 2019. reviewofmm.com/soft-contact-lens-based-myopia-management. 6. Tison K, Parker CB. Add Multifocals to Your Myopia Toolbox. Review of Optometry. 2020. www.reviewofoptometry.com/article/add-multifocals-to-your-myopia-toolbox. |

