 |  |
Brimonidine is an interesting molecule to consider. As an alpha-2 adrenergic agonist, many practitioners may most often think of this medicine for its use in treating glaucoma. The majority of brimonidine’s activity resides in its ability to decrease aqueous production from the ciliary body, though it also helps to facilitate some extra aqueous drainage through the trabecular meshwork. Currently, brimonidine is available in three commercial concentrations: 0.1%, 0.15% and 0.2%.1
So the question is, why would we bring this drug up in a contact lens column? Because brimonidine has an interesting side effect profile that may prove useful to some lens wearers. Due to its activity on the alpha-2 receptor, it also acts to prevent pupil dilation under mesopic and scotopic conditions. This is done via the inhibition of the release of norepinephrine from the pre-synaptic nerve terminal in the cleft of the dilator muscle, which allows the tonus of the sphincter muscle to take over and ultimately reduces the pupil’s size (Figure 1).2 Here, we will discuss three common uses for brimonidine in the contact lens wearer.
Orthokeratology. Some patients are able to wear orthokeratology lenses overnight to facilitate gentle progressive remodeling of the cornea’s shape to remove the need for spectacle or contact lens wear during the day. The most common type of refractive error corrected using orthokeratology lenses is myopia, though advanced designs now also allow for higher levels of astigmatism to be corrected as well via flattening of the central topography of the cornea to create a midperipheral steep curve. This results in a corneal appearance topographically similar to that of a postoperative LASIK cornea (Figure 2).
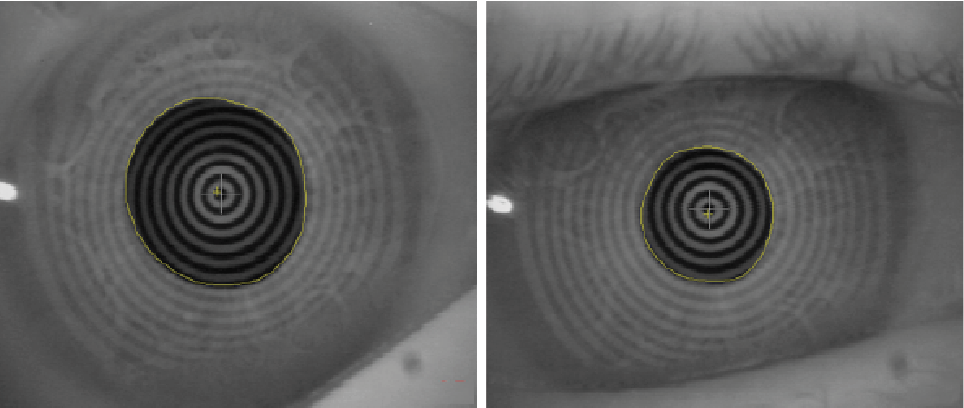 | |
| Fig. 1. (a) infrared pupil readings prior to the instillation of brimonidine; (b) five minutes after the instillation of 0.1% brimonidine. |
But, just as physiological pupil dilation can affect a postoperative LASIK patient’s vision in the evening, so too can it affect a patient who has undergone orthokeratology treatment, as the pupil has the opportunity to dilate out to the edge of the treatment zone in certain conditions, potentially affecting vision. Increasing the size of the treatment zone with modifications to the lens size or decreasing the sagittal depth of the lens can assist with increasing the size of the treatment zone. In this case, one alternative is to have a patient use a drop of brimonidine in mesopic and scotopic conditions where vision may be sub-par.
Multifocal Gas Permeable Lenses. Some of these rigid lenses may at times have their optical zones located on their front surface, while other options will contain some of the multifocal optics on both the anterior and posterior surfaces of the lens. Multifocal GP lenses are typically designed with the distance optics located in the middle of the lens and slowly progressing to the near optics towards the midperipheral and peripheral portions of the lens. Success with multifocal GPs requires appropriate centration both horizontally and vertically. Any significant displacement from the location of the pupil in either of these meridians will affect visual clarity for the patient.
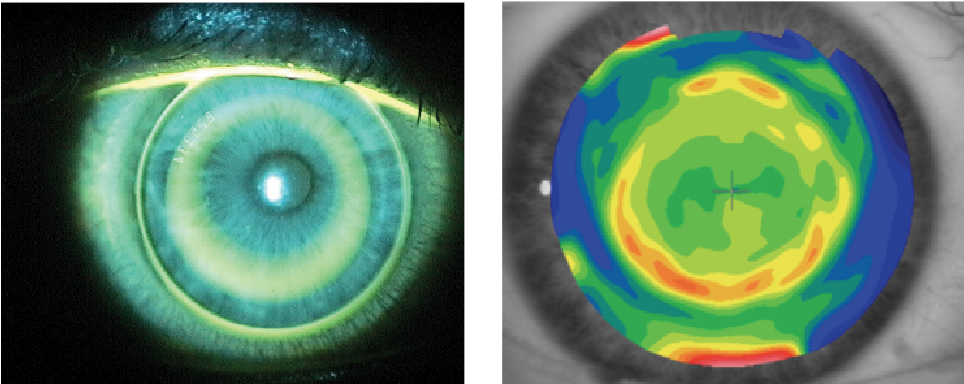 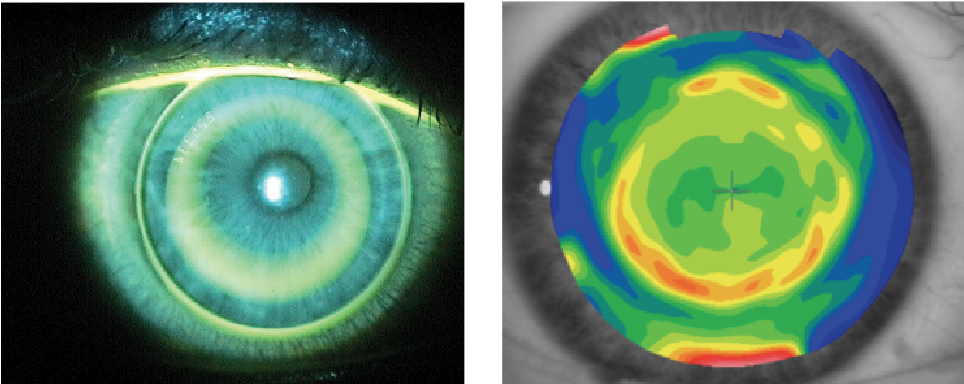 | |
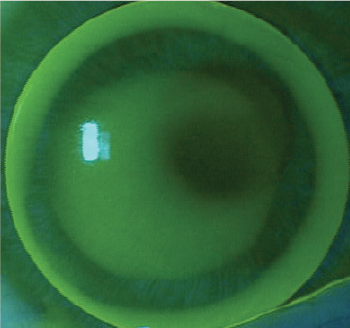
| Fig. 2. Orthokeratology lens on the eye (left) and the topography of the cornea when the lens is removed. |
When appropriately aligned, multifocal GPs provide excellent distance vision and the opportunity for translation into the near optics of the lens. Of course, there are environments that may make the vision somewhat more challenging for these individuals. One example is levels of low light, such as when driving near sunset. Depending on the amount of pupil dilation that occurs in these individuals, their pupils may widen into the region of the lens in which the distance optics begin to transition into the near optics. Fortunately, most GP lens designs can be altered to increase the distance center portion of the lens to allow for pupil dilation with less interference of the near optics.
It is in this case that topical brimonidine may be beneficial as an alternative to moving the zones of the lens to compensate for mesopic and scotopic conditions. This would provide potential visual benefits to the patient without the need to change the properties of the lens itself. Additionally, since the GP lens material won’t absorb the medication, the drug can be applied without removing the lens.
Small Diameter Lenses for Corneal Ectasia. At times, the GP lenses that practitioners fit their irregular corneal patients with are slightly smaller than typical to compensate for how steep the curves on the back of the lenses are. Interestingly, this can create challenges for patients wearing these lenses in the evening, as their pupils may dilate outside of the optical zones of the lenses (Figure 3). In these instances, we can create larger lenses with aspheric back surfaces to compensate. Additionally, semiscleral, scleral and hybrid lenses are often times options for these individuals as well. However, controlling pupil size with brimonidine may also be an option if the patient wishes for the lens characteristics to remain the same.
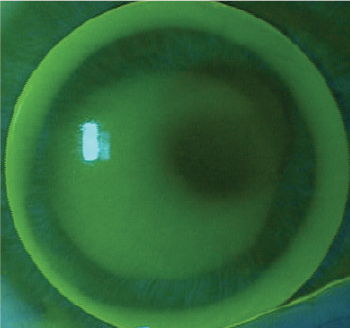  | |
| Fig. 3. Small lens off-center in which the lens edge is approaching the pupil margin nasally. |
Prescribing Habits
Take note that while the above information constitutes suggestions for brimonidine use, minimizing pupil dilation with this drug is not an FDA-approved indication for the product. As such, before proceeding with a prescription for patients in the instances discussed, we feel it necessary to mention this fact to them to ensure they are comfortable using the medication in such a manner. As with any off-label indication, the benefits of treatment must outweigh the risk of adverse events that may result from it. Note, brimonidine use can in some cases lead to dry mouth or a tired feeling.
We typically prefer to prescribe brimonidine in its lowest commercially available concentration, which is 0.1% available as Alphagan P 0.1% (Allergan). We also send instructions with the prescription as follows: Sig: 1 gt OU prn for critical viewing tasks. This statement provides appropriate guidance to the pharmacist that the drug is not to be used on a chronic basis.
Keeping this solution in mind to enhance the vision for those who may be having some difficulties will help enhance their visual outcomes as nothing else can. So, look into it.
1. Allergan. Alphagan P Prescribing Information. Available at: www.allergan.com/assets/pdf/alphaganp_pi.pdf. Accessed May 8, 2016.
2. Shemesh G, Moisseiev E, Lazar M, Kesler A. Effect of brimonidine tartrate 0.10% ophthalmic solution on pupil diameter. J Cataract Refract Surg. 2011 Mar;37(3):486-9.

