 |
Spring always comes with the good—warm weather and outdoor activities—and the bad—ocular allergies. Our offices see a noticeable uptick in complaints of itchy, watery, red eyes and an inability to wear contact lenses comfortably, if at all.
The Problem
Ocular allergies are a growing problem, especially in cities with more air pollution, including hydrocarbons and automotive exhaust.1,2 One study found the rhinoconjunctival tissue of susceptible patients is quite sensitive to irritant stimuli during allergic inflammation, and susceptibility to irritants may increase in areas with more air pollutants.3
Up to 40% of the US population experiences symptoms from ocular allergy: conjunctival chemosis, injection and papillae.4 With up to 51% of patients discontinuing contact lens wear every year, it’s no surprise patients with ocular allergies will drop out of contact lens wear, flooding our practices with unhappy patients and less contact-lens related revenue.5 In fact, the TFOS study proved the conjunctiva to be more closely linked to the development of contact lens discomfort than the cornea.5 The study also suggests alterations of the tear film caused by contact lens wear can cause discomfort.6 A stable and healthy tear film is vital in the defense against allergens, and an allergic eye with an altered tear film allows greater contact time between offending agents and the ocular surface.
Untreated, or undertreated, allergic conjunctivitis can be a direct cause of contact lens discomfort and dropout, and it is our responsibility to identify and treat it quickly.
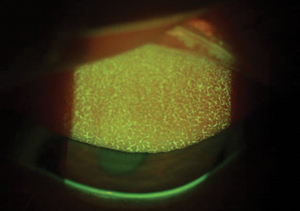 |
| Allergic conjunctivitis can cause significant contact lens discomfort, and must be treated promptly to avoid contact lens dropout. Photo: Jennifer Harthan, OD |
The Solutions
The first step is ruling out other comorbidities such as systemic, corneal, conjunctival or ocular surface diseases, and then alleviating the symptoms of ocular allergy.
Avoiding known allergens is obvious, though not always realistic if the offender is a family pet or home or work environment. Palliative therapies such as cool compresses, artificial tears and fully protective, wraparound eyewear while outdoors all reduce exposure to offending allergens.6 Artificial tears in particular can diffuse or drain away the offending allergen.7 Other therapies include hair washing before bed, avoiding eye rubbing, using HEPA filters and replacing allergen-hosting materials such as pillows and carpeting.6
For patients who require further relief, there are a number of effective over-the-counter (OTC) and prescriptive topical options: decongestants, antihistamines, mast cell stabilizers, combination antihistamine/mast cell stabilizers and “soft” steroids drops. The once-daily dosage offered by some Rx drops is preferable to the four times required by some OTC drops. Topical cyclosporine has also shown promise in the treatment of allergic conjunctivitis.8 Oral allergy agents tend not to be as effective or expedient at alleviating ocular symptoms as topical agents, and can lead to ocular surface drying and the retention of allergens in the tear film.9
For patients who still find contact lens wear challenging, we recommend switching to daily disposables. If this is not feasible, suggest a peroxide-based care system. Daily lenses do not allow offending allergens to bind to the surface of the lens, minimizing likelihood of symptoms. Although a seasonal solution, often monthly disposable wearers opt to continue the daily use modality indefinitely.
1. Wong AH, Barg SS, Leung AK. Seasonal and perennial conjunctivitis. Recent Pat Inflamm Allergy Drug Discov. 2009;3:18-27.
2. Wang P, Thevenot P, Saravia J, et al. Radical-containing particles activate dendritic cells and enhance Th17 inflammation in a mouse model of asthma. Am J Respir Cell Mol Biol. 2011;45:977–83.
3. Riediker M, Monn C, Koller T, et al. Air pollutants enhance rhinoconjunctivitis symptoms in pollen-allergic individuals. Ann Allergy Asthma Immunol. 2001;87(4):311-8.
4. Singh K, Axelrod A, Bieliry L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010;126:778-83.
5. Nicholls JJ, Wilcox MDP, Bron AJ, et al. The TFOS international workshop on contact lens discomfort, executive summary. Invest Ophthalmol Vis Sci. 2013;54:TFOS7-13.
6. Bowling E. What’s trending in ocular allergy treatment. http://optometrytimes.modernmedicine.com/optometrytimes/news/what-s-trending-ocular-allergy-treatment?page=0,0. Optometry Times. January 9, 2015. Accessed April 13, 2017.
7. Trubo R. Seasonal ocular allergy: new options for a recurring problem. Cornea. 2015 Mar:31-3.
8. Wan KH, Chen LJ, Rong SS, et al. Topical cyclosporine in the treatment of allergic conjunctivitis: a meta-analysis. Ophthalmology. 2013 Nov;120(11):2197-203.
9. Raizman MB. Ocular allergy, nasal allergy, and dry eye disease. Advanced Ocular Care. 2010 Mar:48-9.

