 |
Congenital cataracts can lead to deprivational amblyopia in children. However, a good visual prognosis is possible with early detection and removal of infantile cataracts—as long as the subsequent visual rehabilitation with contact lenses is successful.1,2 Children should be fit in lenses that provide the best optical quality and the highest oxygen permeability because the lenses are usually of a high plus power and, consequently, are thicker.
The initial contact lens fitting often occurs during infancy and is sometimes done under anesthesia. Infants are relatively easy to swaddle, which makes taking measurements easier. If the fitting occurs when the child is older, however, ocular measurements can be more difficult to obtain due to a lack of cooperation.
As a solution, creative fitting techniques are designed to help successfully fit these patients in the rigid gas permeable (RGP) lenses they need. This case highlights a method of fitting aphakic bitoric lenses using spherical diagnostic aphakic lenses in a toddler when keratometry (K) readings are unattainable.
 |
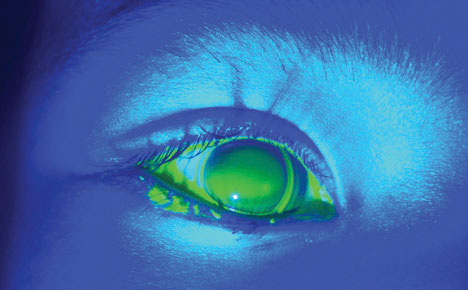
| Fig. 1. To determine this patient’s K readings, I first had to find the flat K. Note the light horizontal band touch with excessive edge lift at the vertical axis. This is a spherical RGP lens fit on flat K: 8.33 BC/10.0D lens. |
The Case
The parents of a two-year-old aphakic child with developmental delay presented and claimed that their child was unable to see clearly in his soft aphakic lenses. They had noticed a decrease in his visual attention and felt he was relying more on his hearing than his sight.
The child had been born full-term but was diagnosed soon after with polymicrogyria, which is a condition associated with abnormal brain development before birth.3 The patient has a history of infantile spasms and is psychologically and physically delayed in his development.
When he was four months old, the child developed cataracts (from an unknown origin) that progressed rapidly within a short period of four weeks. Cataract surgery was performed, and the child was fit with soft spherical lenses that he has been wearing with no issues for the past 16 months.
Currently at 24 months, he does not speak and is not ambulating. He regularly receives behavioral, speech and physical therapy.
During the child’s most recent visit with his pediatric ophthalmologist six weeks ago, findings showed that his eyes had experienced an increase in the amount of cylinder, from 1.00D to 1.75D OU. The child was corrected for full distance in his contact lenses while wearing bifocal glasses to correct for near vision. He currently wears Alden HP 49 lenses at 8.3/+22.00/14.5 OD, 8.4/+20.00/14.5 OS.
 |
| Fig. 2. A 2D steep (7.94D) spherical RGP lens on a toric cornea. |
Contact Lens Evaluation
Subjective visual acuity was not measurable; however, the patient was able to fix and follow OU. Retinoscopy over contact lenses revealed:
- -2.50+2.50x090 OD
- -2.00+2.00x100 OS
On exam, the child’s pupils were equally round and reactive to light; no afferent defect was noted OU. Extraocular muscles were unrestricted in all gazes, and nystagmus was noted. The patient’s intraocular pressures were 11mm Hg OD and 12mm Hg OS, as measured by a Tonopen (Reichert). His anterior segment evaluation was unremarkable. The dilated view of the posterior fundus was also within normal limits, with a cup-to-disc ratio of 0.1/0.1 OU. Due to the cataract surgery, natural lens was absent in both eyes. I did not perform a confrontation visual field exam because of age limitations.
After assessing the patient, I diagnosed him with aphakia OU and progressing astigmatism.
I discussed the pros and cons of three lens options with the patient’s parents:
Soft toric lenses pros: no change in lens modality, familiarity with soft lenses; cons: variable retinoscopy due to soft lens movement, low Dk, not easily verified in-office.
Cylinder-correcting glasses (worn over soft lenses) pros: more control of astigmatism (does not change with rotation), do not dislodge easily, no change in lens modality, familiarity with soft lenses; cons: must be updated to match prescription changes, not as precise optics as RGP lenses,4 soft lenses are not easily verified in-office, low Dk.
Bitoric RGP lenses pros: more consistent retinopathy, high Dk, better optical quality, easily verified in-office, extensive parameters, easy to insert and remove; cons: must learn insertion and removal techniques, more challenging to fit, K readings are not attainable, lens may eject more easily, risk of corneal abrasions.
 |
| Fig. 3. These bitoric contact lenses are properly aligned OU. |
Contact Lens Fitting
The parents were most interested in contact lenses that would provide their son with the best optical quality. Bitoric RGP lenses may be a challenge to fit, but they are the lens of choice when fitting patients with high astigmatism.5,6 K readings were unattainable due to poor cooperation, so I used diagnostic spherical RGP lenses from a Pediasite aphakic fitting set (Advanced Vision Technologies) and fluorescein patterns to estimate the patient’s K readings through the following steps:
Step 1. Determine the flat K reading. Spherical lenses should exhibit band-like astigmatism fluorescein patterns (Figure 1).
Step 2. Estimate the toricity based on the amount of cylinder in the glasses prescription or the amount of edge lift in a spherical lens fitting. A 2D steep spherical RGP lens was chosen as a starting point to reduce vertical edge lift (Figure 2).
Step 3. As outlined in the fitting guide, find the diameter by subtracting 1.0mm from the horizontal visible iris diameter (HVID).
After estimating the K readings, I ordered Pediasite SPE bitoric optimum extreme lenses (Advanced Vision Technologies) with the following parameters:
- 8.33/7.94 (drum reading) +20.00/+18.00 (back vertex power) 10.5 (diameter) OD
- 8.33/7.94 (drum reading) +18.00/+16.00 (back vertex power) 10.5 (diameter) OS
Contact Lens Dispensing
The patient returned, and I placed the lenses on his eyes. I observed good centration, peripheral fit and alignment (Figures 3 and 4). The parents were trained on insertion and removal techniques, which weren’t a problem; in fact, they were able to handle the rigid lenses better than the soft lenses. They were then instructed to use Unique pH multipurpose GP cleaning solution (Menicon) to clean and store the lenses.
 |
| Fig. 4. Above is a close-up of the right eye fit with a bitoric lens. |
Follow-up
Two weeks later, the patient and his mom presented with no new complaints. The child’s visual attention had noticeably improved, according to his mom and behavioral therapist. The patient’s parents were happy with his new contact lenses, and a follow-up appointment was scheduled for six weeks later.
Six years later, the patient is still doing well in his bitoric RGP lenses. Some modifications were made to flatten the lens and change the power as the patient aged.
Discussion
Although they are optically superior to soft contact lenses, RGP lenses can be challenging to fit in young patients due to a lack of cooperation and an inability to obtain K readings. Bitoric lenses can be especially challenging because most are fit empirically.7 While not usually necessary, performing an exam under anesthesia may be required if a child is uncooperative and measurements are unattainable.
For aphakic contact lenses, in-office diagnostic fitting with high plus lenses is highly recommended because these lenses are heavy, which changes the dynamics of the fit and may require clinicians to manipulate the contact lens parameters to achieve better centration. If the cornea is highly astigmatic, bitoric diagnostic sets are not always available. However, as presented in this case, bitoric lenses can be designed using spherical diagnostic lenses.
After determining the flat curvature reading, the practitioner must then determine how much toricity to add by either matching the amount of cylinder in the spectacle prescription or observing the amount of edge lift and lens rock with the spherical diagnostic contact lens. Toricity should be increased if the lens is dislodging or exhibiting excessive edge lift. Toricity should be decreased if the lens is not exhibiting enough movement.4 Against-the-rule corneas should be fit as close to alignment as possible for stability, and with-the-rule corneas can be fit with low toric simulation to allow for adequate tear exchange.7
Ejection, a common challenge with pediatric RGP lens fittings, could occur for a number of reasons. A lens that is too steep will eject on blink and requires a flatter base curve that will need to be adjusted as the child grows. A sudden increase in eye pressure can also cause the lens to eject and should be carefully monitored in aphakic patients. Excessive toricity of the cornea can cause lens rock and decentration. In this case, a clinician should fit the patient in a bitoric lens or increase the toricity of the current lens. For heavy lenses that displace easily, the optic cap size or center thickness of the lens should be reduced.8 Lastly, the diameter should be large enough to optimize lens stability.
Spherical diagnostic contact lenses are valuable tools for fitting both spherical and bitoric RGP lenses on infants and children when K readings are unavailable. When managing aphakic lenses in young patients, the optic cap, lens thickness and diameter size can be manipulated by clinicians to improve stability and centration. Although initially more challenging, RGP lenses can provide more stable and precise vision for young patients. As these children age, clinicians should consider a secondary lens implantation for better results.
|
1. Taylor D, Vaegan, Morris JA, et al. Amblyopia in bilateral infantile and juvenile cataract. Relationship to timing of treatment. Trans Ophthalmol Soc UK. 1979;99(1):170-5. 2. Neumann D, Weissman BA, Isenberg SJ, et al. The effectiveness of daily wear contact lenses for the correction of infantile aphakia. Arch Ophthalmol. 1993;111(7):927-30. 3. Chang BS, Piao X, Giannini C, et al. Bilateral generalized polymicrogyria (BGP): a distinct syndrome of cortical malformation. Neurology. 2004;62(10):1722-8. 4. Silbert J. Rigid contact lenses and astigmatism. Contact Lens Practice. 2nd ed. London: Butterworth-Heineman Elsevier. 2005:488-514. 5. Sarver M. Visual correction with contact lenses. Clinical Refraction. 3rd ed. Chicago: Professional Press, 1977. 6. Weissman BA, Chun MW. The use of spherical power effect bitoric rigid contact lenses in hospital practice. J Am Optom Assoc. 1987;58(8):626-30. 7. Hom M, Bruce A. Manual of contact lens prescribing and fitting. 3rd ed. Missouri: Butterworth-Heinemann. Elsevier. 2006:227-34. 8. Lindsay RG, Chi JT. Contact lens management of infantile aphakia. Clin Exp Optom. 2010;93(1):3-14. |

